
Causes of Shortness of Breath that should be considered in the Emergency Department
22nd February 2022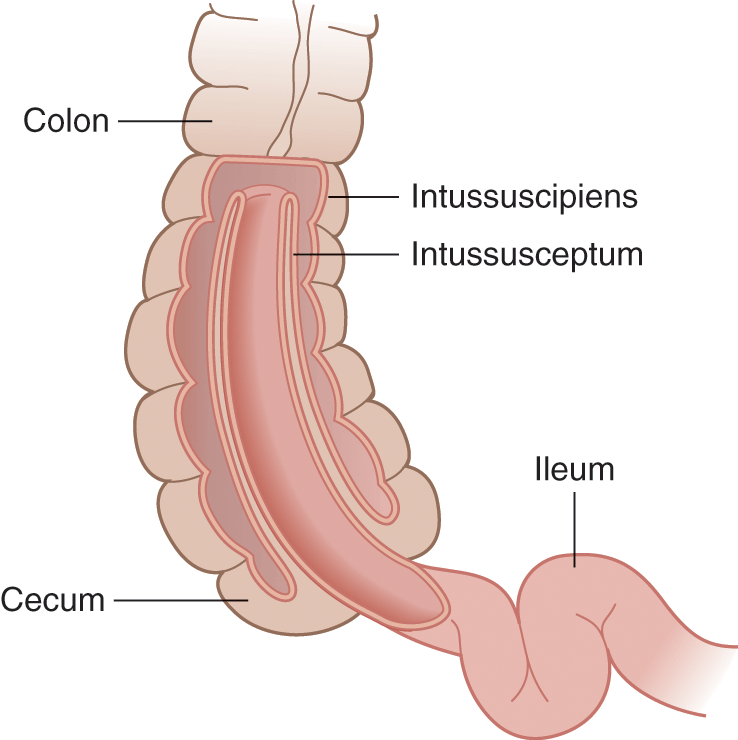
Intussusception as a cause of abdominal pain in children
9th March 2022
When a patient arrives in the emergency department complaining of chest pain, it’s essential to rule out red flags as rapidly as you can. Their life might depend on it. These possible reasons for chest pain have been explored before (link to earlier article).
At the same time, though, physicians and medical professionals should not rush to diagnose severe cardio-pulmonary illnesses, such as heart disease. Doing so could result in improper investigations and treatment and increase the risk of clinical negligence claims.
There are other causes of chest pain which also need ruling out before proceeding to other possible diagnosis avenues:
Cause #1: asthma
Asthma is a common condition, affecting 8% of the adult population. Asthma occurs due to inflammation in the airways as a result of an autoimmune response which can, in some cases, lead to chest pain.
Presentation in the emergency department can be similar to cardiovascular complaints. Patients may be struggling with shortness of breath and oxygenating their tissues.
To test for asthma, perform a physical examination. Listen for signs of wheezing, indicating obstructed airways although in severe disease the chest may e silent with little air movement. Check for swollen nasal passages and a runny nose. Perform a peak expiratory flow (lung function test) to see how well the lungs are working.
Cause #2: hiatus hernia
Hiatus hernia can result in chest pain when part of the stomach pushes up against the chest cavity. It is a common condition and can lead to symptoms that look similar to serious cardiovascular disease.
To diagnose a hiatus hernia, may require investigations under the care of gastroenterologists but if the Emergency Medicine clinician considers that the patient they are reviewing has this condition rather than a cardiovascular emergency they can discharge the patient back to their GP for ongoing investigations
Cause #3: panic attack
Panic attacks are common and can result in symptoms associated with serious cardiovascular diseases, such as elevated heart rate, chest pain, dizziness, sweating, and nausea. However, symptoms are transient.
To diagnose a panic attack, perform an ECG to check the electric function of the patient’s heart. While the doctor may suspect that the patient has a panic attack as the cause of their presentation to the Emergency Department they may be difficult to diagnose without admission and investigations including Troponin levels and observation for a period.
Cause #4: myocarditis
Myocarditis, or inflammation of the heart muscle, can result in chest pain, fatigue, and trouble breathing. Unlike conventional heart attacks, however, patients often present with a fever.
To diagnose myocarditis, perform a blood panel to confirm elevated troponin, creatine kinase and white blood cell levels that might indicate damage to the heart muscle. Determine whether the patient has antibodies and other blood factors associated with bacterial and viral diseases of the heart. Again often myocarditis requires invasive procedures to make a tissue diagnosis under the care of the cardiologist.
Cause #5: muscle strain
Inflammation of the intercostal muscles in the ribcage can cause severe, acute chest pain. Pain may become worse with activity, causing patients to present at the Emergency Department. It can also be provoked in some patients by a vigorous episode of coughing.
Ask the patient if the pain gets worse with activity. Get them to point to where their pain is most intense and perform a physical examination. Point bony tenderness even to gentle palpation of the patient is a good clinical sign of a Musculo-skeletal problem.
If such a problem has cause a fracture of a rib, and this can be difficult to distinguish from a soft tissue injury the patient can develop a pneumothorax and in those circumstances a chest X-ray should be performed.



{kind=link}
{kind=link}
{kind=link}