
Expert Struck off – A salutary lesson
28th April 2020
Managing an expert medico-legal practice and remote working
11th May 2020Cauda equina syndrome and a medico-legal responsibility
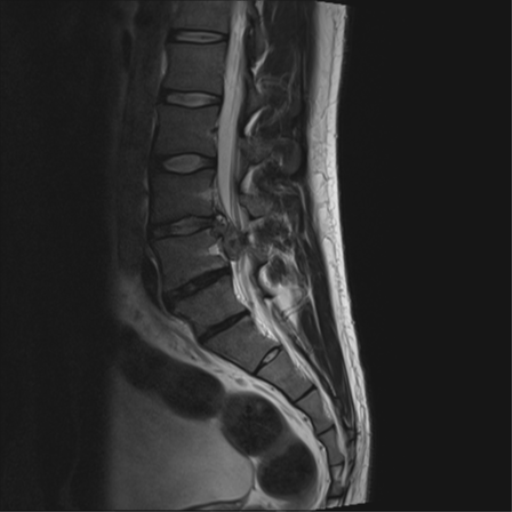
Case courtesy of Dr Henry Knipe, Radiopaedia.org. From the case rID: 53615
Cauda equina syndrome, where multiple nerves are compressed in the lower spine causing bladder and bowel dysfunction, is a serious condition.
When the syndrome is fully developed it is easy to diagnose but unfortunately the outcome if the diagnosis is made at that time is at best variable and at worse there is no improvement of symptoms.
It is however much more difficult to make the diagnosis of the condition especially among the group of patients who present to the Emergency Department with back pain often having had the back pain for a period of time.
The Getting it Right First Time ( GRIFT) initiative undertaken by NHS Improvement included Spinal services in its remit and this was published in January 2019.
This stated that any patient with back or leg pain with any disturbance of bladder or bowel function or sensory disturbance in the saddle or genital area or bilateral leg pain should be suspected to have possible or actual cauda equina syndrome.
One of the problems with reporting on such patients who present to the Emergency Department and are discharged before returning with clear symptoms is that there may be a difference between the history and examination as recorded in the medical records and the recall of the patient in their witness statement.
Sometimes it is obvious that the clinician has not asked, or more correctly recorded in the notes, pertinent questions and the answers about altered sensation or alterations in urinary symptoms but other times these questions are recorded in the negative in the notes but the patient maintains there were both symptoms and they informed the doctor at the consultation.
As an expert you must not make decisions about the facts and whether the symptoms were complained of, asked about or recorded incorrectly.
You must give an opinion based on what the court finds and therefore more than one opinion may be correctly given depending on what factual decisions are made by the court.
The key investigation in suspected or actual cauda equina syndrome is an MRI scan and the GRIFT report indicates that should be performed before referral to a spinal centre.
While most hospitals with Emergency Departments have an MRI scanner this may not be available 24 hours a day and may require a senior referral to have this done in an emergency.
For the Emergency Department where the diagnosis of cauda equina syndrome is only suspected in a patient presenting in the late evening this may require the patient to be admitted overnight for the investigation to be undertaken the next day and this requires the patient to be referred to an in-patient team who may be reluctant to admit the patient.
In a patient with clear signs of cauda equina syndrome where no immediate local MRI scan is available then referral to the local spinal service should be undertaken as they are likely to have access to MRI scanning 24 hours a day.
For the clinician taking a comprehensive history including recording explicitly the answers to questions about altered sensation and bowel and bladder problems and undertaking a full examination including of perianal and genital sensation is important.
For the expert, noting any differences between the medical records and the notes and giving opinions on both will show they have the independence and understanding of their duty to the court.



{kind=link}
{kind=link}
{kind=link}