
Assessing the patient in the Emergency Department when they are intoxicated
16th March 2021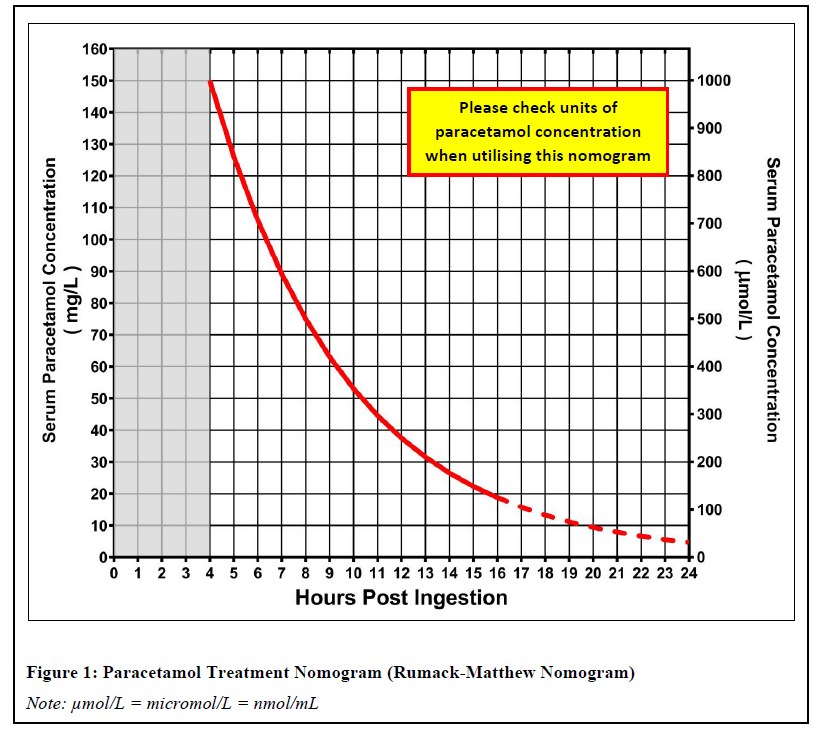
Paracetamol overdose: how to avoid medical negligence claims
2nd April 2021
I have previously written about the dangers of missing an ectopic pregnancy in the Emergency Department but pregnant patients also present to the Emergency Department later in their pregnancy to the Emergency Department.
In those patients a different set of diagnoses need to be considered and indeed both the care of the patient and their unborn child are of importance when deciding on the need for treatment and whether there needs to be input from the obstetric team in addition to any other specialists involvement.
There is a maxim in the Advanced Trauma Life Support Course that good care of the foetus is best served by good care of the mother and I would contend that this principle extends to other non-traumatic presentations of pregnant patients to the Emergency Department.
Pregnancy causes physiological changes in the patient most obviously in the last trimester and the increase in uterine size also displaces organs in the abdomen meaning that the normal landmarks of clinical signs of common diseases such as appendicitis are displaced.
Patients can also present to the Emergency Department with medical conditions such as chest infections or possible Deep Vein thrombosis that may require hospital admission.
In those circumstances involvement of the obstetric team in conjunction with he admitting medical team may require the patient to move to a hospital site where there is a Consultant led obstetric service if their local hospital does not have such a service.
Abdominal pain in the pregnant patient
There are however conditions that cause abdominal pain, which are pregnancy-related. Apart from the risk of ectopic pregnancy in early pregnancy in later pregnancy, there are numerous possible causes for abdominal pain. These include a uterine tear, a ruptured uterus, and an acute fatty liver (AFLP). It’s necessary to ascertain whether the patient has had previous surgery on the uterus (C-section or myomectomy) as this increases the likelihood of a secondary uterine rupture.
There are causes of abdominal pain unrelated to pregnancy which either require surgical or medical intervention. If untreated, these conditions can complicate pregnancy.
Acute appendicitis is the most common non-obstetric surgical emergency during pregnancy – cholecystitis and pancreatitis closely follow. The typical presentation of acute appendicitis alters depending on how far the patient is in her pregnancy. Pain normally localises initially in the periumbilical area and then spreads to the lower right quadrant. Guarding is not as common in pregnancy so relying on the lower right quadrant for diagnosis is advised.
The pregnant patient may have other conditions which only require medical intervention, such as deep vein thrombosis and sickle cell disease.
Managing the pregnant patient in the Emergency Department
To successfully manage pregnant patients, one must ascertain immediately whether the patient’s condition is urgent or non-urgent. This involves checking for haemodynamic stability, cardiovascular stability, respiratory distress, and if there’s a traumatic injury to the abdomen. The obstetrics team also uses the Early Warning Score, which is accurate in identifying women at risk of dying. (Paternina-Caicedo, et al., 2017)
While patients who have obstetric causes for their attendance at the Emergency Department need urgent referral to the obstetric team the Emergency Medicine medical staff may be focused on the primary need for surgical or medical referral for the primary problem that they forget that monitoring the foetus is an important part of their assessment of the whole patient in the Emergency Department and such a review can alert them to any deterioration in the condition of the foetus while still managing the mother.
While the medical team may refer the mother to the medical or surgical team in a timely manner the nurses should involve the midwifery team even if there is a non obstetric cause for the attendance at the Emergency Department.
In many circumstances pregnant patients will have no ill effects on the foetus if the Emergency Department follow the maxim of treating the mother well but by reassuring the mother by monitoring the foetus at he same time as providing that care will reduce any adverse effects on the foetus.



{kind=link}
{kind=link}
{kind=link}