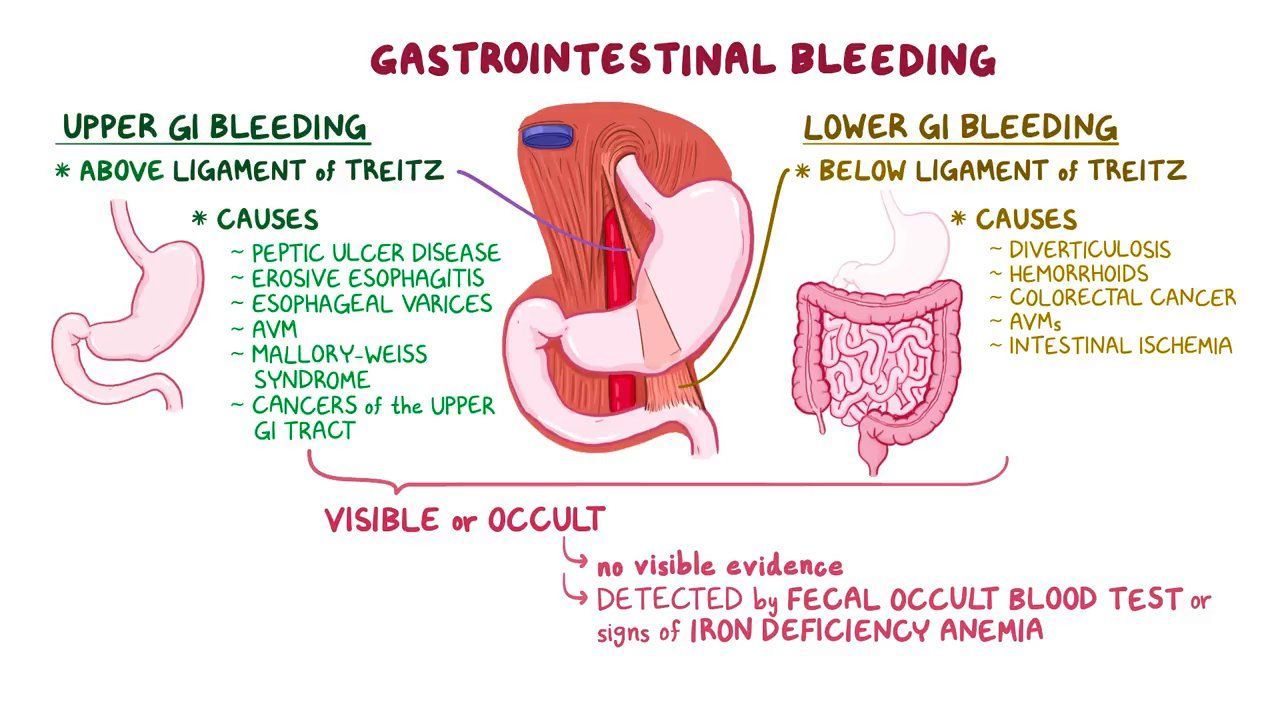
Upper GI Bleeding In the ED
9th February 2021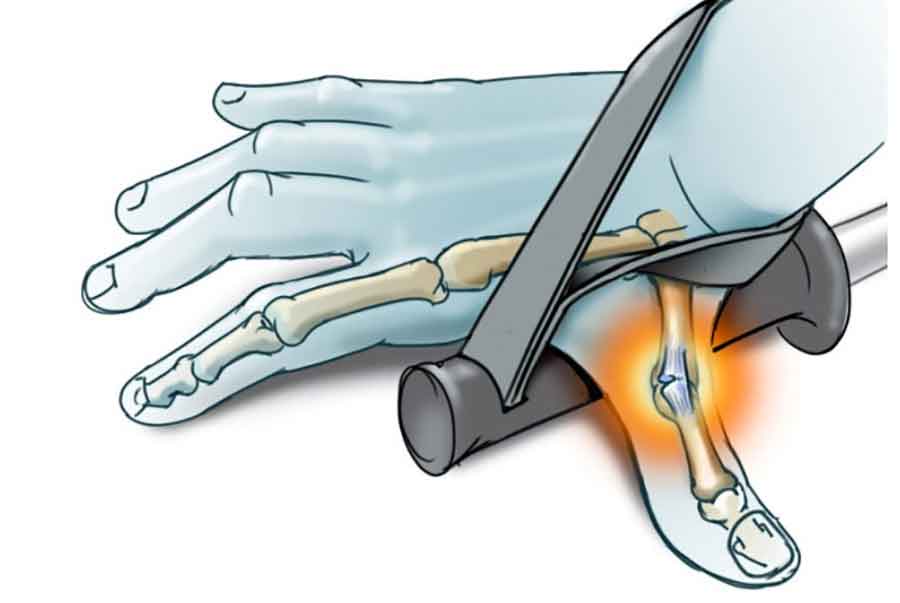
Skier’s Thumb in the ED
1st March 2021
Meningococcal disease presents as either meningococcal septicaemia, meningococcal meningitis, or both. Any of these diseases carry fatal implications for the patient if left untreated.
Meningococcal septicaemia is a bloodstream infection caused by the bacteria Neisseria meningitidis. Upon entry, the bacteria multiply in the bloodstream and damage endothelium, causing bleeding into the skin and organs. Septicaemia can then spread to the meninges, resulting in bacterial meningitis.
There are other types of septicaemia caused by different bacteria, such as pneumococcal and Group B Streptococcal. Further, viral and fungal septicaemia can also occur. Therefore, identifying the true cause of septicaemia is crucial for effective treatment.
Without immediate diagnosis and subsequent treatment, the prognosis is poor for meningococcal septicaemia – life-changing defects, such as limb loss, may result. If treatment is delayed too long, death will result. If treated early, most children and adolescents – the most affected cohort – make a full recovery. (NICE 2008)
Diagnosing & Managing Meningococcal Septicaemia
Upon admission, the patient may present with typical signs of septic shock, including fever, chills, vomiting, hypotension, and tachypnoea. The patient may also show changes in mental signs – a common indicator of bacterial septicaemia.
Later signs include a petechial rash, but this often arises too late for effective treatment and should not be used to make a diagnosis. The glass tumbler test is one quick diagnosis test – the rash fails to fade when the glass is pressed against it.
To see if the patient has also developed meningococcal meningitis, the clinician may use the Kernig’s test or Brudzinski’s test – both of which detect pain in the meninges. If the patient is losing consciousness, a CT scan might identify increased intracranial pressure.
If the clinician suspects meningococcal septicaemia, they must perform laboratory investigations. These investigations involve two EDTA tubes for meningococcal DNA using PCR and blood cultures. A negative PCR test will not rule out N. meningitidis. However, the clinician should not await results before starting treatment.
If the patient is under 16, they must receive ceftriaxone intravenously at the earliest opportunity. The clinician will also provide fluid resuscitation, seizure management (if necessary), and respiratory support.
If the patient is over 16, they must receive IV antibiotics, such as penicillin or ceftriaxone, at higher dosages. Management protocol for adults then follows – similar to that in children.
The Implications Of Delayed Diagnosis
Symptoms of meningococcal septicaemia within a short time frame are life-threatening. The patient, within hours, can fall into a coma and consequently suffer from lasting after-effects or death.
To prevent the spread of meningococcal, prophylaxis is necessary. If the patient has become infected in a social setting, it’s important to identify those that the patient came into contact with. Currently, ciprofloxacin is recommended as a prophylaxis for those who might be infected. (PHE, 2017) This is especially the case for children in school year groups or students in university halls.
Unfortunately, patients with delayed diagnosis now live with neurological defects, internal organ damage, and permanent limb loss. Therefore, a quick, or even suspected, diagnosis is vital to save a patient’s future welfare or their life.

{kind=link}
{kind=link}
1 Comment
[…] Meningitis remains a high‑stakes medical emergency, carrying a mortality risk of approximately 1 in 6 and long‑term disability in up to 20% of survivors . Delay or deviation from best practices—such as postponing lumbar puncture (LP) or failing to initiate prompt antibiotic therapy—can result in worsened neurological outcomes or mortality, which in turn can trigger medico‑legal claims. […]