Acute Kidney Pain: Is It A Stone?
11th January 2021
Toxic Shock Syndrome in the ED
27th January 2021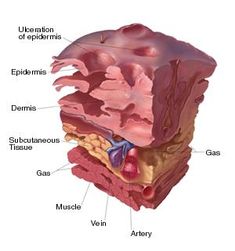
Necrotising fasciitis is a rare but often fatal bacterial infection that occurs beneath the skin and around the muscles and organs. One particular type of necrotising fasciitis is sometimes known as “flesh-eating disease’, where the name stems from bacterial toxins that damage nearby tissue.
Bacteria can enter the body through a wound, minor or significant, to trigger necrotising fasciitis. However, there is not always a point of entry.
There are three main types of necrotising fasciitis: type 1 (polymicrobial); type 2 (haemolytic group A streptococcus/staphylococcus, such as MRSA); and type 3 (gas gangrene caused by clostridium). Type 1 is often seen in elderly patients or patients affected by diabetes or other conditions. Type 2 affects all age groups, healthy or otherwise. Type 3 usually follows surgery or injury whereby gas is trapped under the skin, causing crepitus.
Necrotising fasciitis starts deep in nature, perhaps due to an infected suture or secondary to trauma, and works upwards towards the skin surface. Therefore, it is important to remember that necrotising fasciitis may not always be obvious on the surface. Type 2 is particularly aggressive and triggers exotoxin-driven toxic shock syndrome, which can initiate significant multi-organ failure and thus requires rapid treatment to prevent patient mortality.
Often the diagnosis is delayed as the early clinical signs are often non specific and the Emergency Medicine clinician has to have a high index of suspicion where the clinical signs appear not to show an obvious source of illness or infection
The Royal College of Emergency Medicine provides guideleins that the clinician should consider the following risk factors: advanced age, diabetes, immunosuppression, obesity, drug abuse, severe chronic illness, skin injury, and malignancy. Further, observing early (fever, malaise) and late (crepitus, purple discolouration, and septic shock) clinical signs aid in diagnosing the stage of necrotising fasciitis.
Management for Necrotising Fasciitis
Upon diagnosis, the clinician should take an aggressive approach to treatment. Necrotising fasciitis may require immediate surgical input to save the affected limbs or life. Involvement in the early management of patients by a surgeon is important and the Emergency Medicine team should alert a senior surgeon as soon as the condition is suspected
Immediate initial resuscitation by the Emergency Department will ensure the tissues are well-perfused and receiving adequate oxygen to prevent the development of multi-organ dysfunction. The patient will receive IV crystalloid solution to treat potential vasoplegia and oedema in the affected area. In case multi-organ failure does occur, invasive blood pressure monitoring and central venous access is required for potentially necessary inotropic support and may require the involvement of the ITU team.
The clinician should also administer broad-spectrum IV antibiotics as soon as the microbiologist identifies the cause of necrotising fasciitis. Antibiotics should prevent septic shock if administered early enough in necrotising fasciitis development. Clindamycin is considered if Type 2 necrotising fasciitis is suspected.
Whilst the patient is undergoing treatment, the patient should be admitted to an ITU under the management of a multidisciplinary team or after initial surgical treatment. Once the patient has stabilised and the infection has cleared, specialist reconstructive surgery may proceed to improve significant deformities which resulted from debridement.
Though necrotising fasciitis is rare, it carries life-threatening complications. Thus, it is vital to reiterate that necrotising fasciitis requires consideration with very high clinical suspicion.


{kind=link}
{kind=link}
{kind=link}
1 Comment
[…] while infiltration injuries can be caused by other solutions that do not result in blistering or tissue death. Infiltration injuries often result in soreness, redness, and swelling around the site of […]