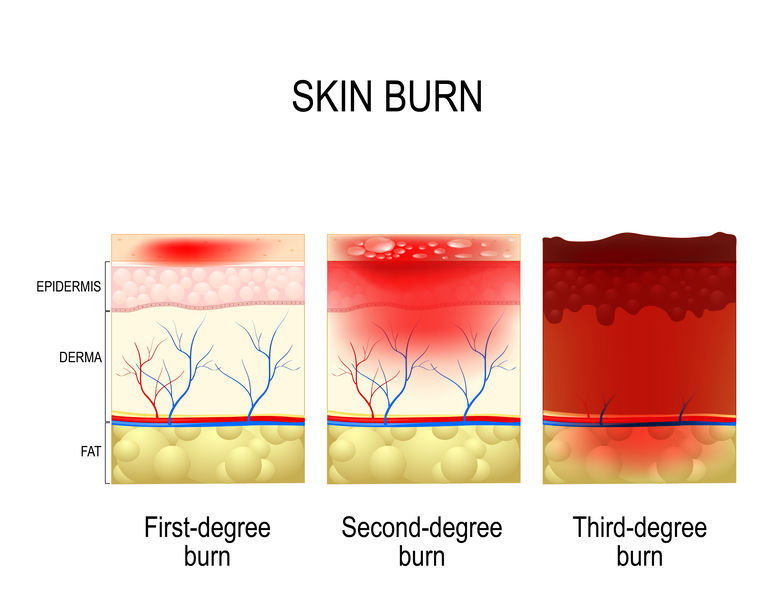
Burns pitfalls in the Emergency Department
29th September 2020
“Side Hustle” or Business
12th October 2020
Acute aortic dissection (disruption of the medial layer of the wall of the aorta) can be easy to miss in the Emergency Department (ED) but requires immediate treatment in order to minimise risk and increase chances of survival. A recent investigation conducted by the Healthcare Safety Investigation Branch (HSIB) found that a delay in the diagnosis of aortic dissection occurs in 16-40% of cases. Moreover, HSIB determined that even with a diagnosis, 50% of patients die before reaching a specialist centre. (HSIB, 2020) These statistics are a stark indication that the diagnosis and management of aortic tears needs much improvement.
The most common symptoms of acute aortic dissection are chest and back pain, sometimes accompanied by confounding neurological symptoms. This fact may lead ED clinicians to initially suspect a cardiac cause for the pain, thus contributing to diagnostic delay. Another complicating factor is that the condition can be easily missed on x-ray, ECG or ultrasound; while these tests are being run, the patient can suffer from irretrievable consequences, again, due to the diagnostic delay. Fortunately, there are several factors that, if considered early enough, can prove lifesaving.
Think aorta
When a patient presents with severe, unexplained pain in the neck, back, chest or abdomen, a clinician should at least consider the possibility of aortic dissection. There are some features of the pain that can help differentiate aortic dissection form myocardial infarction. In the case of the former, the pain is usually abrupt and maximal at the time of onset and can migrate as the dissection progresses. This contrasts with the slow-building, duller pain caused by myocardial infarction.
Consider risk factors
It serves the clinician well to be aware of the signs and symptoms of aortic dissection, including which populations are more at-risk for this malady. Research shows that between 50-75% of patients with dissection have or have had hypertension. (Thrumurthy, et al., 2011) Men, especially ones aged 60 and above, are much more likely to suffer from dissection than women or younger adults. Risk factors can also include a history of smoking, high cholesterol or pre-existing aortic disease or a family history of it.
If the patient cannot be treated in the hospital that they present to there is a balance between undertaking investigations to confirm the diagnosis and transferring the patient to the specialist centre for treatment. In these circumstances early consultation with the thoracic or vascular specialists to confirm whether urgent transfer is more important that confirming the diagnosis by imaging
Conduct imaging
It is not always possible to conduct diagnostic imaging in emergency situations, however, if imaging can be carried out, a rapid CT scan is the best option, as recommended by the HSIB report, for confirming a dissection diagnosis.
A diagnostic delay for a patient with aortic dissection can prove fatal. Therefore, it is essential for ED personnel to develop better protocols and have strong knowledge of possible risk factors that could indicate dissection. A clinician’s ability to consider the various contingencies when treating a patient in the ED ensures that the standard of care is met and can lead to lifesaving interventions


{kind=link}
{kind=link}
{kind=link}
1 Comment
[…] aetiologies, including acute coronary symptom, pulmonary embolism and thoracic aortic dissection (which I have discussed in a previous article). For a patient describing the sudden onset of these symptoms, without a history of recent trauma, […]