
Correct Diagnosis and Treatment of Hand Injuries
18th August 2020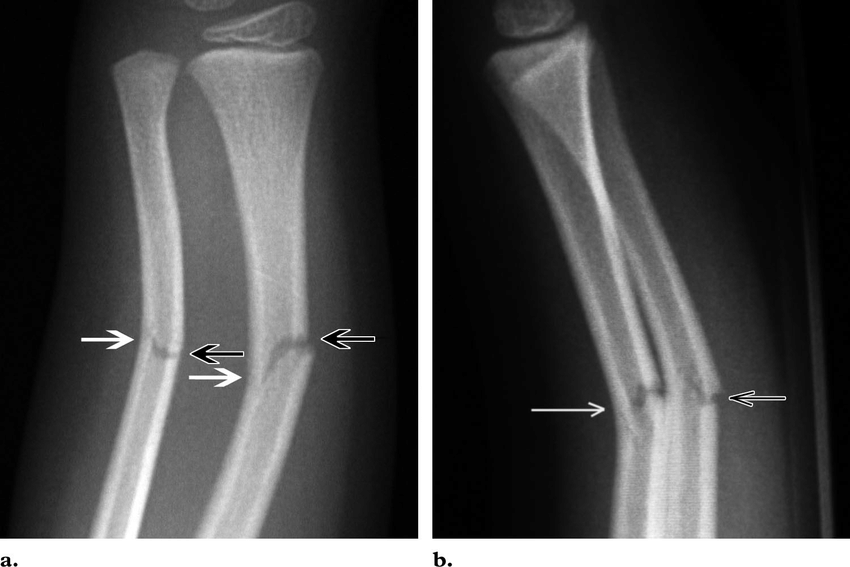
Paediatric fractures: distinctive features of the immature skeleton
2nd September 2020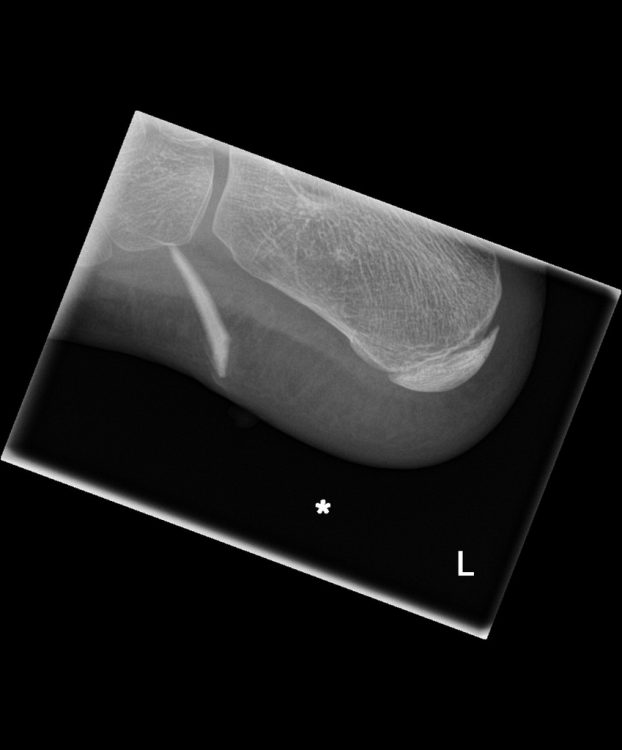
Patients presenting to the Emergency Department (ED) with soft tissue wounds are a common occurrence. One imperative of the attending physician is to carefully assess these wounds for possible retained foreign bodies (FB). One retrospective study found that in approximately 38% of patients with soft tissue wounds in the hand, foreign bodies were missed upon initial assessment, often because imaging was not undertaken. (Anderson et al., 1982) An undetected FB can cause long-term complications such as infection, nerve and tendon injuries or bone necrosis and chronic pain.
In some cases, wounds contaminated by foreign material can be cleared by irrigation or by extraction with instruments in the ED, when they are visible. Identifying a concealed foreign body may prove more difficult; but there are indicators that make the presence of an FB more likely. A patient may not initially suspect an FB is present and a visual examination may be inconclusive. Knowing that an FB is more likely following penetrating injuries or abrasive trauma means that an important step in the initial evaluation is to determine the mechanism of injury in addition to the type and location of the wound.
Initial imaging and wound exploration should be considered if an FB is suspected. Plain radiographs are relatively inexpensive and pose little radiation risk. Radiopaque materials such as metal and glass are most easily detected through radiography. On the other hand, vegetative materials, such as wood, absorb bodily fluids, making them more difficult to spot through imaging. These materials could be diagnosed through ultrasonography but require a skilled technician. (Rupert et al., 2020) and to undertake such an investigation for all wounds would be an onerous undertaking with little rewardd
Exploration and removal should be discussed with the patient, with risks and benefits clearly outlined. In some cases, an FB can be left in place if it is inert (certain metal, glass or plastic objects), not causing discomfort and is located away from vital structures. However, the FB should be removed, either in the ED or by a specialist, if the risk of complications is high, which is often the case with organic FBs or sharp foreign bodies in the digits. Deciding whether removal should take place in the ED or the patient should be referred to a surgeon depends on the difficulty of the case, depth of penetration and possibility of complications. (Skinner & Morrison, 2020) and a junior Emergency Medicine doctor should ask for a senior review before leaving a foreign body in situ.
A clinician must be familiar with the different possible types of foreign bodies and the appropriate imaging techniques. This knowledge will help determine the urgency of the situation, the necessity of removal and whether specialty referral is required.
This systematic approach can reduce complications caused by foreign bodies in the skin, such as possible infection and delayed healing that can lead to chronic pain or further injury to the patient.
It is also important if a wound is not explored to give appropriate advice to the patient when they are discharged about the indications that there may be a retained foreign body and when they should seek further medical attention


{kind=link}
{kind=link}
{kind=link}