Foreign bodies in the skin: identification, exploration and removal
26th August 2020
How to get paid: strategies for receiving timely payments for your medicolegal work
9th September 2020
The paediatric skeletal system is unique in that it allows for rapid growth and change. The main differences between the paediatric and adult skeletons are that the bones have to allow growth as the child matures and therefore there are growth plates normally at the ends of the bones where an area of cartilage to allow the growth. These distinctive features can lead to specific patterns of injury more common in children than in adults. Some of these can present diagnostic challenges. The Emergency Department physician should be aware of the particularities of the paediatric skeleton and the age specific changes that occur in bones and the types of fractures that can occur, especially as pertains to epiphyseal fractures (growth plate fractures). Although complications from growth plate injuries are uncommon, failure to recognise and manage them properly may lead to growth arrest and long term deformity.
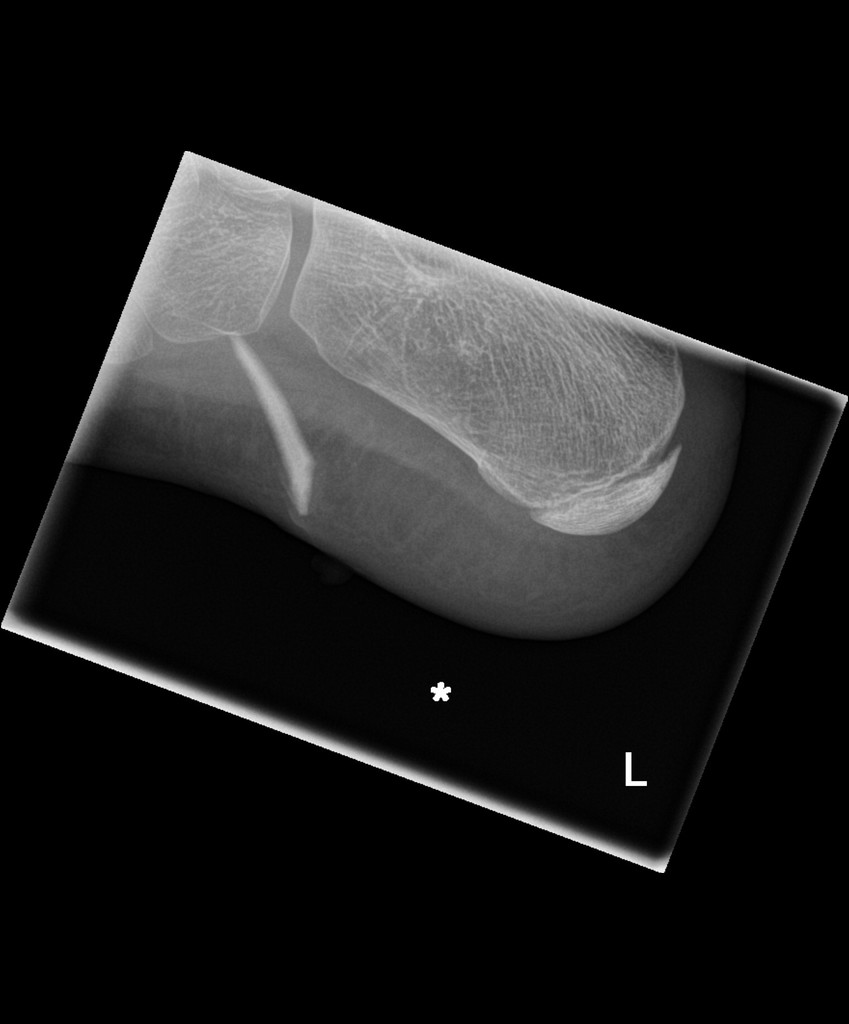
Two type of fractures are specific to the paediatric skeleton and result from the bone’s ability to bend before breaking; these are the torus (“buckle”) and greenstick fractures. Failure of a child’s bone in compression usually results in a buckle fracture. These fractures most commonly occur in the distal metaphysis ( the main part of the bone), where porosity is greatest. They are generally stable and pose minimal displacement risk. (Williams et al., 2018) Indeed there is often no need to treat in plaster. Greenstick fractures are characterised by a bending injury with a fracture line that does not completely go through the bone. Because of their instability, greenstick fractures present a high risk of re-fracture and require rapid immobilisation. These types of fractures also require orthopaedic follow-up. (Atanelov & Bentley, 2020) Both of these fractures can be diagnosed relatively quickly if the physician knows what to look for. As always, obtaining a detailed history (including mechanism of injury) and conducting a thorough physical examination (to determine exact location of suspected fracture), before obtaining radiographs, are essential for a correct diagnosis. The best way to make the diagnosis on X-ray is to look for sudden alteration in the contour of the bone which is not usual in bones.
One of the diagnostic pitfalls for paediatric fractures in the ED, is that more complex fractures, involving epiphyseal plates, could be missed or mis-diagnosed as a torus, greenstick or other type of fracture. Epiphyseal fractures represent between 15% and 18% of all pediatric fractures, however, they may not be visible on a radiograph due to the low density of the cartilage that makes up the growth plates. Another consideration is that an injury to an adult that might result in a sprain or joint dislocation often results in a fracture to a child. Therefore, it is important to at least consider an occult growth plate injury before diagnosing a sprain.
Some basic knowledge about these fractures can help the emergency physician arrive at the correct diagnosis. For example, growth plate injuries are most common during periods of rapid growth and often occur in a predictable pattern. Research has found that approximately 80% of such injuries occur between the ages of 10 and 16 years. They are more frequent in boys than girls. The distal radius is the most common anatomic site of growth plate injury, accounting for 30% to 60% of cases. (Perron et al., 2002)
The history and physical examination are the most valuable pieces of information when it comes to physis injuries. Different mechanisms of injury can indicate specific types of growth plate fractures. For example, a fall on outstretched hand (FOOSH) is a typical mechanism for physeal injuries to the distal radius. Point tenderness over a physis can be another reason to suspect this type of injury. The Salter-Harris classification system is commonly used to categorise epiphyseal fractures based on anatomy, fracture pattern, and prognosis. This classification is important because patient treatment and follow-up are strongly dependent on the type of fracture The ED clinician should be familiar with characteristics of each classification. While type I and II injuries may be managed by immobilisation, elevation and rest, a type III injury requires an orthopaedic consultation because of the need for near-perfect re-alignment. The higher the Salter-Harris fracture classification number, the greater the chance of serious complications. (Cepela et al., 2016) Unfortunately type I (1) and type V (5) cn look identical on X-ray but have very different prognosis.
In conclusion, a clinician must be familiar with the distinctive features of the paediatric skeleton and how these can affect injuries and fractures. Moreover, the ED clinician should maintain high suspicion for growth plate injuries in paediatric patients presenting with fractures. Although the complications brought on by epiphyseal fractures are relatively rare, early detection and management further minimises the risk.



{kind=link}
{kind=link}
{kind=link}