
Expert Struck Off: An Update
30th July 2020
Foreign Bodies in the Eye: what is the extent of injury?
10th August 2020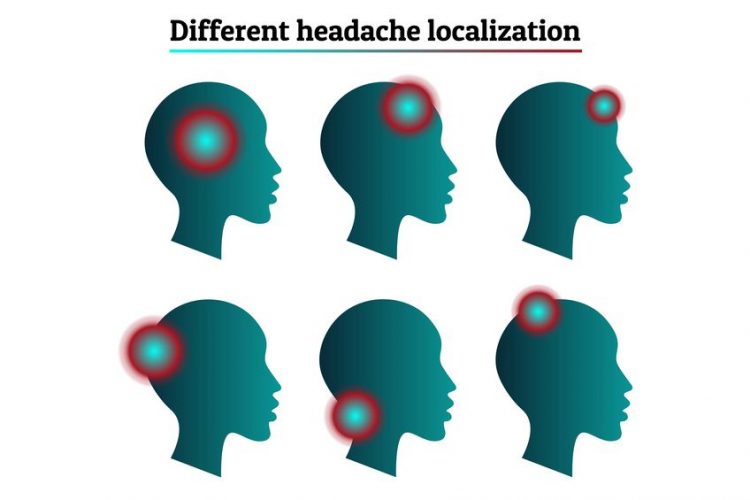
Patients presenting to the Emergency Department with a chief complaint of acute headache are a relatively common occurrence. A headache can be a symptom of many systemic illnesses but should not be discounted as an important clue when assessing the patient. As with other clinical scenarios in the ED, a thorough and systematic approach is essential in arriving at a correct diagnosis and ensuring swift treatment for the patient. Even though most headache complaints in the ED are likely benign, it is important that the attending physician be able to recognise the signs of potentially life-threatening scenarios that begin with a sudden and severe headache.
As stated above, most headaches are due to benign primary headache disorders; these include tension-type headaches, migraine headaches, cluster headaches and headaches stemming from medication overuse. However, the consequences of a more serious, undiagnosed, condition underlying the headache can be devastating. A clinician in the ED must maintain the precarious balance between recognising these more severe pathologies, while also limiting unnecessary investigations. To this end, NICE provides a guideline meant to improve recognition and management of headaches, provide targeted treatment and reduce unnecessary investigation. In most cases, getting a thorough history of the patient will identify primary headache disorders, thus eliminating the need for further investigation and allowing the clinician to focus on management and treatment. Therefore, ED physicians must focus on identifying the headaches stemming from life-threatening pathologies, which can be broadly categorised into structural, infectious and vascular. (Akhter et al., 2019)
Red flags that indicate the need for further investigation would normally emerge during an initial assessment and history. Fever or recent antibiotic use could indicate possible meningitis. Neurological deficits, syncope or seizures could mean elevated intracranial pressure, which could be the result of encephalitis, an intracranial abscess or a central venous thrombosis. Obtaining a patient’s cancer history (previous malignancy) as well as whether they are immunocompromised (for example due to HIV) are important factors in making a diagnosis as well, as patients with this type of history at higher risk for life-threatening pathologies. Moreover, patients over the age of 50 may be at higher risk for secondary headaches caused by acute ischaemic injury or cerebral venous thrombosis. The clinician’s main role is to rule out any of these life-threatening causes for a headache and be aware of the signs and symptoms that do warrant further investigation. (Kennis et al., 2013)
In assessing a case involving a patient who presented to the ED with a headache, an expert must first determine whether the attending physician took thorough history and carefully assessed the patient and documented any decisions made regarding further investigation and treatment.


{kind=link}
{kind=link}
{kind=link}
1 Comment
[…] decreased vision in one eye with a headache over the affected eye which the patient says becomes worse when chewing. Experiencing pain, fatigue […]