
Meningococcal Septicaemia: The Dangers Of Delayed Diagnosis
16th February 2021
Why An Expert Witness Needs A Website
9th March 2021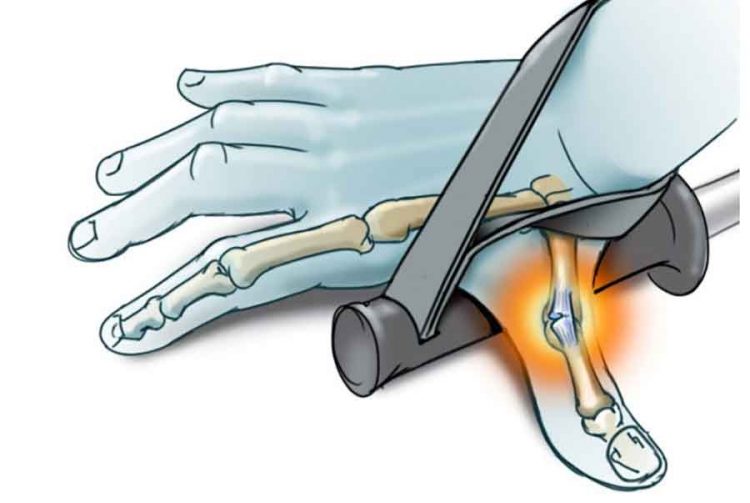
Injuries to the ulnar co-lateral ligament (UCL) of the thumb are usually caused by forced abduction of the thumb away from the rest of the hand. In the past one of the forces that could cause such a stress on the thumb was using forearms and that was how the injury was given the name of Gamekeepers thumb. Now one of the more common causes is with falling while on the ski slope and is particularly seen on artificial slopes where the thumb catches in the matting and has led to the injury being renamed Skier’s thumb.
The ligament can be injuries at either of its attachments to the proximal phalanx of the thumb or the metacarpal where it may pull (avulse) a small bony fragment that is visible on X-ray or it may be injured in substance of the ligament where no bony abnormality would be visible.
If left untreated, chronic injury to the thumb UCL can increase the patient’s risk of joint instability, loss of pinch strength, and painful movement in use.
In the majority of cases, conservative management of UCL injury leads to complications. A Stener lesion may arise, where the adductor insertion into the metacarpal interposes between the divided ends of the ruptured UCL. This lesion prevents the ligament fragments from remaining in proximity where some healing may occur but with the ends separated by the tendon of another muscle no healing can occur.
It is therefore important to make the diagnosis of this injury and institute treatment as leaving the injury untreated may lead to long term instability and joint problems.
Investigating Thumb UCL Injury
The patient may present with pain and swelling at the base of the thumb, which is a more common presentation for acute UCL injury. If the injury is chronic, the thumb will show signs of weakening and potential deformity. The patient may not always present with pain, and joint instability is more indicative, especially when accompanying a Stener lesion.
The common presentation of joint instability associated with a damaged UCL is the first point of investigation. Valgus stress of the MCP joint may reveal laxity. The clinician should test laxity in both a neutral position and when the MCP is fully flexed – this position isolates the UCL. If there’s a difference in angulation between the two thumbs, this shows a positive test for UCL injury. If the patient complains of pain when stressing the joint this is unlikely to be a complete rupture of the ligament but may be a partial rupture that if not recognised and protected can lead to a complete disruption later.
It’s important to note that a physical examination of the thumb joint may displace an avulsion in the affected area and worsen the injury. If this is suspected, imaging should be performed first to diagnose an avulsion fracture.
Simple X-rays may or may not identify an avulsion fracture fragment wither form the proximal phalanx of the thumb or the tip of the metacarpal but sometimes the X-ray may not show a fracture at all.
An X-ray taken when stressing the joint may show that the joint line widens on the ulnar side as the ligament cannot hold the joint in situ. While an ultrasound may show disruption of the ligament often the exact degree of damage may not be found until definitive treatment occurs at operation.
Treating Thumb UCL Injury
Partial and complete tears to the UCL require different management strategies.
A partial UCL injury is normally treated with conservative management. This is especially the case if the patient suffers from degenerative MCP joint disease. Patients should meet the following criteria to pursue this course of management: no fractures, less than 30 degrees laxity in the MCP joint, and no larger than a difference in 15 degrees in laxity between the two thumb joints.
In conservative management, a thumb spica containing a thumb splint immobilises the thumb MCP joint. The patient should be discharged from the Emergency Department to the care of the orthopaedic or hand surgery service.
If there is a complete disruption of the ligament or a fracture on the X-ray the patient should be referred the same day to the on call hand surgery team or their consideration of operative treatment and follow up.



{kind=link}
{kind=link}
{kind=link}