
Managing an expert medico-legal practice and remote working
11th May 2020
The Medico-Legal Expert’s Knowledge of Guidelines.
26th May 2020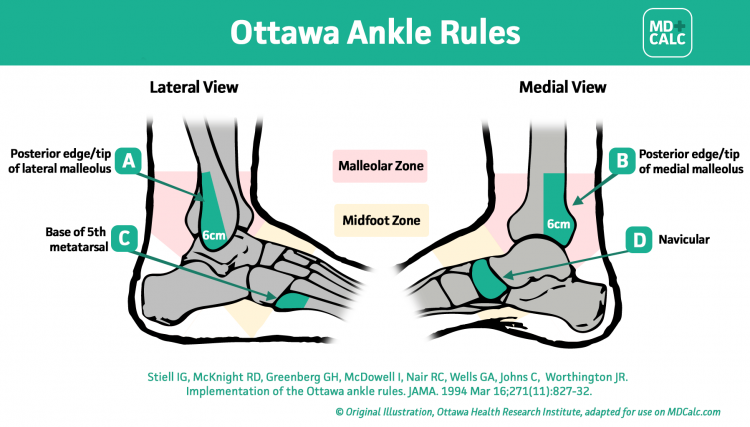
Previously, I talked about the scaphoid fracture and how this can be missed in the Emergency Department.
However many other fractures can be unidentified in the Emergency Department normally when a clinician does not undertake an X-ray or X-rays the wrong area of the body.
How then can a clinician be sure to identify a fracture clinically without exposing every patient to radiation.
The Royal College of Radiologists undertook a study asking clinicians to document the clinical signs in patients and correlated these with the outcome of X-rays.
They came to the conclusion that if one or more of obvious deformity, point bony tenderness and inability to weight bear in the lower limb or significant loss of function in the upper limb were present, this would identify over 90% of significant fractures that would alter treatment.
These guidelines then became enshrined in written guidelines and can be used when addressing if an X-ray should or should not have been undertaken in an individual case.
However even using these guidelines common injuries, such as a sprained ankle, still would mean excessive numbers of X-rays where many would be negative.
This has led to the development of certain rules such as the Ottawa Ankle rules which limits the areas of bones that tenderness is needed to warrant an X-ray and also makes a quantitative number of steps that the patient needs to undertake (less than 4) to mandate an X-ray.
The advice is as follows:
- If ankle pain is present and there is tenderness over the posterior 6 cm or tip of the lateral or medial malleolus, then ankle x-ray is indicated.
- If midfoot pain is present and there is tenderness over the navicular or the base of the fifth metatarsal, then foot x-ray is indicated.
- If there is ankle or midfoot pain and the patient is unable to take four steps both immediately and in the emergency department, then x-ray of the painful area is indicated.
The Ottawa Rule makes clear that for those who fulfil none of the advice, then an ankle or foot X-ray is not required. However, if a patient fails the criteria in some way, then clinical judgement is required.
There is still a need for the expert to be sure that the records clearly documents the examination that has been carried out and that it meets the criteria for an X-ray not to be undertaken.
Often what can happen is that the clinician has made a diagnosis before undertaking a full examination including the whole of the lower leg rather than just examining the ankle thus missing a fracture higher up the leg.



{kind=link}
{kind=link}
{kind=link}
4 Comments
[…] mentioned previously in my post about indications for X-ray in fractures one of the key determinants is whether the patient can weight bear with a lower limb […]
[…] have previous written about fractures and why it is important for the clinician to assess patients fully and if required undertake […]
[…] giving a history of their ailment, a patient with a painful joint may erroneously link the pain with a minor injury that they suffered recently. The medical team […]
[…] common issue with this type of injury is that it can be misdiagnosed as a sprained ankle – a thorough diagnosis must be carried out so that the clinician can carry out the right […]