
Differential diagnosis of the limping child
18th January 2022
Patients presenting with suspected drowning in the emergency department
31st January 2022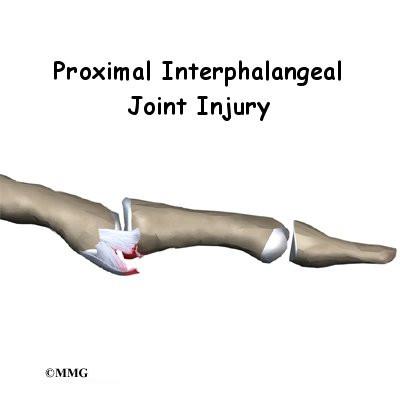
Hand injuries are one of the most common problems that present in the emergency department. Subtleties in the clinical findings of hand injuries can result in misinterpretation and an incorrect diagnosis. It is also the case that clinicians are more often presented with injuries to the arm and shoulder than to the finger, which can result in less familiarity in diagnosis and treatment. Not recognising volar plate injuries of the hand can result in profound functional loss, significant pain and stiffness of the finger from early osteoarthritis.
The volar plate and common injuries to it
The volar plate is a strong, thick ligament that connects two bones in the finger. It is one of the structures that stabilise the proximal interphalangeal (PIP) joint. The volar plate prevents the finger from being bent backwards under normal conditions.
Often known as a ‘jammed finger’, the volar plate is usually damaged by the finger being bent too far backwards (hyperextended). It can also be caused by a crush injury to the PIP joint. In severe cases, the finger joint can be dislocated. When a fragment of bone is dislodged in such an injury, this is known as a volar plate avulsion fracture.
Symptoms of a volar plate injury
The most common symptoms of a volar plate injury are immediate pain in the vicinity and a loss of motion in the joint as well as swelling and bruising. Bruising will usually be most noticeable around the middle joint of the finger. There may also be an observable loss of pinch power between the finger and thumb.
An examination of the patient’s history will often reveal a forced hyperextension. Volar plate injuries are common among athletes – particularly ball sports that involve catching, contact sports, and those that involve jumping and landing.
Diagnosis of a volar plate injury
Diagnosing a volar plate injury will involve a physical examination and analysis of the patient’s history. A radiograph will usually be required and will also be used to diagnose a volar plate avulsion. The appearance of radiographs of volar plate avulsions can vary markedly between cases which can lead to a higher probability of misdiagnosis.
There are several classification systems for volar plate injuries. The two most often used are Eaton’s and the Kiefhaber-Stern classifications. The resulting conclusion from the use of either scale will indicate whether a conservative management programme is recommended or whether the injury will require surgery.
Treatment of a volar plate injury
Conservative treatment plans for a volar plate injury will usually involve extension-blocking immobilisation of the PIP joint with a splint. This is usually achieved by ‘buddy splinting’, where the injured finger is taped to a healthy neighbouring digit. There are various surgical options for more severe or complex volar plate injuries. These include volar plate arthroplasty and screw fixation of the volar fragment.
Hand therapy and recommended gentle exercises will usually follow treatment and typically begin within a few days of treatment at the hospital. Full motion is usually achieved following a volar plate injury. However, for some patients, if the injury has also damaged the collateral ligaments alongside the volar plate, there may be continued swelling at the joint which may never go away.



{kind=link}
{kind=link}
{kind=link}